Back To Basics with Nasolabial Folds and Marionette Lines
9th March 2017 | Dermal Fillers
In this article we go back to the basics to discuss Nasolabial folds and Marionette lines.
Nasolabial Folds are the lines that run from the corner of the nose to the corner of the mouth, and marionette lines are the lines that run from the corners of the mouth down to the chin. People often notice them as being the first visible signs of an ageing face and often present to an aesthetic clinic to have them corrected with injections of dermal filler.
Treatment of Nasolabial folds or Marionette lines (also known as puppet lines) used to be the most requested dermal filler treatment in our aesthetic practice. The reason I’m calling this article back to basics is because treatment of these two indications with dermal fillers are quite literally the first thing Emma and I, as well as countless other practitioners ever learnt to do when we started in aesthetic medicine. Personally my first 500 treatments were almost certainly just Nasolabial lines and Marionette lines. In the 11 years since Emma and I started practising aesthetic medicine there have been significant milestone developments in our understanding of the anatomy, physiology and psychology of ageing. This has led to a shift from filling these areas specifically, towards a more holistic global facial rejuvenation using multiple techniques in addition to dermal fillers.
The reason we initially changed our approach is because we understand that for the majority of our patients, replacing facial volume globally, rather than specifically to one area creates a more natural rejuvenated look. We’ve been thinking a lot about this recently in Clinetix. We have noticed over the past few years a desire amongst our patients still have nasolabial and marionette correction even after full facial volumetric correction. And this really does make a face seem more youthful, when done well.
The traditional approach for this area of simply filling the skin crease and revolumising the subcutaneous tissues will invariably lead, with repeated and excessive treatments, to a flattening of the natural contour of the face. An unnatural and unaesthetic outcome.
The beauty of reflecting back on our practice now, is that now we can see where we weren’t getting it quite right, and now we can see exactly how we can do it to get the all important natural “untreated” looking aesthetic. We can do this now because of two major developments. Firstly our understanding of the anatomy of the area allows us to correct volume loss exactly where it happens. Secondly the technological developments in dermal fillers mean that we now have medical devices (dermal fillers) that can provide natural looking and feeling results.
Now when a patient requests filler in the nasolabial fold, we appreciate that it really is a fold, not a line. It should be there to an extent and completely lifting it out looks unnatural. Now we get that, we can think of the techniques and fillers we are going to use to lift it back to a natural position.
Drs Simon and Emma Ravichandran are Nationally recognised experts in aesthetic medical treatments and run training courses in medical procedures including nasolabial fold and marionette line treatments from their base at the Aesthetic Training Academy in Glasgow as well as other venues throughout the UK.
Aesthetic Medical Training at Clinetix
9th November 2016 | Dermal Fillers
This weekend we ran another of our small group bespoke aesthetic medical training sessions. As someone who has been through the training processes involved in becoming a doctor, and then the training involved in specialisation, Dr Simon Ravichandran has some clear ideas on the methodology required to achieve optimum training outcomes.
The goal of any training is to give the delegate the skills and knowledge to modify or improve their practice, and to give them the inspiration and direction to develop further learning pathways for themselves. Quite often aesthetic medical training courses are conducted as “pathways of entry” into the field. Equipping delegates with the bare minimum required to commence a practice in aesthetic medicine. Thus courses are often overly subscribed, with large numbers of delegates attending to see a days worth of lectures and demonstrations in order to collect a certificate that can be used as a “passport” to practice.
The difference with Clinetix training courses is that Dr’s Simon and Emma Ravichandran are passionate about their speciality, passionate about their patients, and passionate about their teaching. Our goal is not to produce “competent” practitioners, but to produce inquisitive and inspired practitioners who have the ability to go forward and continue to develop in their chosen field.
In order to get the best out of training, delegates require to be able to closely observe treatments, and to perform treatments under close observation and supervision. For this to work well the ratio of instructors to delegates has to be low, ideally less than 3 delegates per instructor.
Last weekend we ran a bespoke training course for two delegates, a Doctor and a Dentist who were both actively practising aesthetic medicine. The aim was to lift the level from basic line filling and wrinkle chasing to an appreciation of the ageing processes of the face, and the techniques we can use to personalise the treatments to the individual face, rather than provide a list of treatments from a menu.
It was a great couple of days covering the use of toxins for the muscles in the lower face and neck, and dermal fillers in the mid face, temples and perioral area. Also the use of new techniques such as using a cannula to treat a lip instead of making a series of injection with needle with the risk of bruising and swelling.
One of the delegates commented on the lip treatment “Well there’s no going back now I’ve seen that!”
Clinetix Training Academy runs a series of courses in aesthetic medicine from foundation courses to introduce people to the speciality through to masterclass courses to demonstrate the latest and most advanced techniques and technologies. If you are interested in learning more about aesthetic medical training at Clinetix you can e-mail us at courses@clinetix.co.uk
Multi-Modal Treatment Planning For Natural Looking Aesthetic Rejuvenation (Or how we get it right! )
2nd November 2016 | Thread Lifts
Anti-wrinkle injections weakens muscles, we know that. But ageing is multifactorial, not just a product of muscle over activity. To create natural looking aesthetic rejuvenation it stands to reason that we need more than just anti-wrinkle injections to keep us looking younger. Obvious isn’t it! Yet we still find that anti-wrinkle injections is the worlds number one requested cosmetic treatment.
Here’s a picture of me taken recently, you can ignore the beard, that’s gone now 🙂
Anti-Wrinkle Injections can relax the lines and wrinkles on my forehead, if I had any there. It can also smooth lines and wrinkles around my eyes and between my eyebrows, likewise if there were any there. However, it’s not going to help overall with making me look and feel a bit younger. In fact, if I had nothing but anti-wrinkle injections for the next ten years I’d start to look decidedly odd! With a smooth and wrinkle free upper third of my face but quite an aged appearance to everything else.
What I am seeing when I look at this image is the deeper shadow developing at the side of my nose, the hollowing at the cheek at the side of my mouth, the wrinkling of the skin underneath my eye and the flattening of my cheek underneath the eye. If I was being super critical I’d probably also mention some very early volume loss just above my eyebrow that will probably develop over time and make my eyes look a bit more skeletal. For the sake of a complete picture I can also see a receded hairline and marked thinning of the hair on the top of my head. That’s what more than ten years in Aesthetic Medicine will do to you!
The answer is clearly not just anti-wrinkle injections.
Let’s think about a real person now, a typical prospective aesthetic patient who presents to a clinic just like Clinetix wanting to look and feel refreshed and rejuvenated. Lets assume it’s a female patient right in the middle of the age range of people who attend my clinic about 45. When she sits down in front of me and tells me she feels her appearance makes her look and feel tired or depressed I don’t reach immediately for the wrinkle syringe, I reach for the mirror and ask her to point to what is causing her concern.
These days it’s getting less likely for the fingers to be pointing at the crows feet, or the frown lines. Instead they generally go to the middle and lower parts of the face first, indicating sagging skin, jowl formation, downturned mouths with thin lips and changes in skin quality like roughness, pigmentation or large pores. We consider these features as part of a holistic rejuvenation process in order to create better results for our patients.
Creating Natural Looking Aesthetic Rejuvenation with a Multi-Modal Treatment Plan
As ageing is multifactorial we approach rejuvenation with a multi-modal treatment plan. This means we can use a wide variety of treatments to address individual aspects of ageing together to create a synergistic and harmonious natural looking rejuvenation.
The Volumetric Approach To Facial Rejuvenation
I like to visualise the ageing face from the bottom up. Think of an old house that’s sitting on dodgy foundations. The roof is falling apart and the window frames are all broken. I can fix those things easily but the house will still be sinking on it’s foundations. Therefore there’s not a huge amount of point other than for the temporary cosmetic fix. For a long term fix you need to start with the foundations to build a house that will last.
The foundation of the face is the bones of the skull and the dense layers of fat that sit above. As we age we get specific changes in the shape of the skeleton, areas that flatten and regress. We also get reduction in the amount of dense fat that overlies it. Most of my consultations begin with an assessment of the foundations of the face and a plan to replace that lost volume. The volumetric approach to facial rejuvenation. With a detailed understanding of the anatomical changes of the skeleton with ageing, and the availability of safe injectable implants (dermal fillers) we create a plan to inject in specific areas to restore a natural shape to the deep face.
This will build up a strong support upon which the upper layers of the face can be more naturally restructured. The amount of dermal filler required to achieve such a correction varies with age of the patient. However it is usually fairly predictable using the formula 1cc per decade of life plus 1cc. This means that someone in their mid forties will usually require 5 syringes, someone in their mid fifties may require 6 and someone in their mid thirties may require 4. We place the dermal filler in the areas of the face to give maximum support as required for the patient. Typically these areas are the cheeks, the temples, the side of the nose and the jawline.
Lifting Jowls and Sagging Skin
The next area of concern is the more superficial fat layers of the face, these can be smoothed with softer, less lifting dermal fillers to correct irregularities and improve contour. But when sagging of the skin and early jowl formation become a concern then we often need to think in terms of re suspending the user layers. The traditional approach to achieve this is the surgical facelift. However, the advent of safe and effective thread lifting techniques now gives us a non-surgical alternative.
Threads are introduced through small holes made with a needle at the side of the face and placed into the upper layers of the faced. Using a thread called a PDO Cog, we can place a fan of threads that can be gently pulled. This creates a lift and repositions the upper layers of the face. This technique is very effective at lifting the upper fat layers of the face. Which in turn has an effect on the appearance of nasolabial lines, marionette lines and jowls.
Rejuvenating the Appearance of the Skin
Once we have revolumised and lifted the face the final thing to consider is the skin. There are many many different ways to rejuvenate the appearance of the skin and the decision will depend on the desired result, the budget and the desires of the patient to have a quick result with one or two treatments, or a more gradual process with several skin treatments over a period of time. With our non-surgical rejuvenation packages we offer CO2 Laser resurfacing or Chemical Peels to get rapid and dramatic results. We also have a range of specially designed combination skin treatments that treat multiple layers of the skin using different techniques at the same time for improved results with no downtime.
Laser Resurfacing
Laser resurfacing or Fractional Ablative resurfacing uses a high powered laser to cause controlled damage to the skin at a specific depth. The skin responds by creating more healthy collagen and more ground substance in the dermis. This results in firmer and more resilient skin. The epidermis is also resurfaced providing a fresher and more lustrous skin with less blemishes, pigmentation and surface irregularities. The recovery period following a laser treatment is about a week. Initially your skin will be red and it is likely to take some time to heal afterwards.
Chemical Peels
For Chemical peels there are many many options but for a rapid result we recommend a medium depth TCA peel. This is a solution that is applied skin and allowed to soak through the deeper layers of your skin. The TCA causes a controlled damage to the dermis at a specific layer. The skin above this layer then peels off over the course of a week as healthier fresher skin grows underneath.
To summarise, a complete facial rejuvenation treatment plan should consider all the signs of ageing. It should also be able to address each one separately in order to achieve a natural aesthetic result.
Our goal is to make our patients feel better about the way they look. In turn make them feel more confident about themselves as a whole! The goal is never to make someone look like they have had a treatment. After a treatment people should be complimenting you about your appearance, but they won’t know what has changed. As I often say to my patients, if anyone asks you who your Doctor is, come and tell me because it means I’ve done something wrong. If they ask you if you’ve been on holiday or changed you hair then we’ve got it right!
If you’d like to have a chat with Dr Simon or Dr Emma Ravichandran about a personalised treatment plan, get in touch here or give us a ring on 0141 221 0229 for our West End clinic or 01698 854 221 for our Bothwell clinic.
The Differences in Rejuvenation Approaches Between the Male and Female Face
23rd September 2016 | Male Rejuvenation
This article is aimed mainly at medical aesthetic practitioners but we hope that you find it interesting if you read to the end. This article details the differences between male and female rejuvenation approaches. If you have any feedback or questions on the article please contact us on info@clinetix.co.uk
Introduction
In current non-surgical aesthetic practice we are seeing a steady increase in the number of male patients presenting for aesthetic rejuvenation treatments. The number of men in the United States seeking botulinum toxin injections increased by 268% between 2008 and 2011 [1]. There have been a number of suggested explanations for this rise, including a growing desire for men to appear more youthful and therefore competitive in the workplace and an increasing social acceptability for such procedures. Whilst the trend is ongoing, the majority of patients in aesthetic practice are still female. This means that busy practitioners who frequently see large numbers of aesthetic patients become very familiar with the female aesthetic, whilst remaining less familiar with the male aesthetic. Unfortunately this shift in skill to the female side means that the male patients are often receiving substandard or inappropriate treatments, as it is clear that the male form differs from the female, and accordingly an approach to female rejuvenation and beautification will not result in a satisfactory outcome when applied to a male face.
In todays competitive aesthetic market, where practitioners find themselves competing with less trained and non-medical service providers delivering the same treatments over and over again it is vital that the expert stands above the rest and differentiates his or her practice on superior quality, by offering expert techniques that deliver outstanding results based on superior knowledge.
In order to develop the skills required to provide outstanding aesthetic rejuvenation treatments in both men and women, an understanding of sexual diamorphism is required, coupled with a profound appreciation of both male and female beauty. This article aims to outline the differences between male and female facial anatomy, and their relevance to aesthetic rejuvenation procedures. This is intended as a guide rather than a set of instructions, to allow the reader to subtly alter their approach between male and female patients, and modify their techniques accordingly. We split the article into segments detailing specific areas, which when taken as a whole will allow a holistic appreciation of the subtle differences in anatomy and accordingly treatment.
The Forehead:
Often the last approached area in non-surgical facial rejuvenation, the forehead, is actually one of the most important areas where marked differences are seen between the sexes. Anthropologists studying skulls use the skeletal structure of the forehead as a significant indicator as to the sex of the skeleton[2] The forehead begins at the supraorbital ridge inferiorly and runs superiorly to the hair line. The female skeleton characteristically has a flat supraorbital ridge with a smooth convexity running up to the hairline, the male skeleton however has a prominent and more projected supraorbital ridge, above which is a concavity before it flattens out and becomes concave again. This convexity gives rise to the appearance of supraorbital bossing in males. The prominent supraorbital ridge is medially continuous with the glabella giving rise to a more pronounced and projected glabella region in males. [3] This skeletal difference gives rise to three important sexually defining characteristics, the prominent glabella and supraorbital bossing as described, but also the skeletal structure influences the overlying soft tissues and thereby the postition of the eyebrows. The male eyebrow sits along the supraorbital ridge and is generally flat [4], whereby the female brow starts medially in the same position, but arches superiorly at an angle of between 10 and 20 degrees with the tail more superior to the head.[5]
The goal of aesthetic medicine is to restore a youthful and importantly natural appearance, So the techniques that we apply to a female patient, such as forehead revolumisation or brow lifting with neuromodulation and revolumisation may result in a feminized and unnatural appearance if used injudiciously on a male patient. Our guide when approaching the male forehead is to elevate a ptotic brow with neuromodulation and fillers if required, but endeavour to lift no more than the supraorbital ridge. An extensively bossed forehead is an indicator of volume loss and should be corrected, but there should remain a small element of bossing that corresponds to a natural contour. The female brows are more amenable to lifting techniques, and the forehead should be revolumised, when required, to acheive a smooth and natural looking convexity to the hair line.
The Cheek:
The cheek is an extensively covered area with regards to aesthetic rejuvenation and the literature is awash with descriptions of the female contour and the female rejuvenation process, however very little is said of the male cheek. Even with the availability of literature and advice on female cheek rejuvenation we all frequently see poor treatment outcomes, seemingly from the repetition of the same cheek inflation treatment over and over again, with a consequent deformed and overinflated appearance. The cheek from an injectable perspective is largely a soft tissue structure, overlying the maxillae medially, the zygoma laterally and the deep fat and buccinator muscle inferiorly. Whilst some maxillary and zygomatic resorption does occur with age, more so in males than females [6], it is the overlying soft tissue contours that give rise to the characteristic differences surface contours between the male and female cheek. Overall the ideal female cheek is believed to be rounder and fuller, whereas a male cheek is flatter and more angular [7]. A pair of studies using MRI to quantify the differences in subcutaneous facial fat in men and women and their changes with age [8,9] showed that overall the male face has a thinner layer of subcutaneous fat, but also that whilst the distribution of fat in the male cheek is uniform, the female cheek has a thicker fat compartment in the medial area as compared to the lateral area, with a ratio of 1.5 to 1. This uneven distribution explains why the female cheek is rounder and fatter, and the male cheek is flatter, conforming more to the contours of the underling structures.
The anatomic approach to a natural rejuvenation should respect the relative anatomy and thus for a male the subcutaneous should be filled uniformly, replacing the lost volume and maintaining the flatter and more angular cheek contour. For a female rejuvenation the volume replacement technique should be the same, but the volume of product used should vary, with more placement medially to mimic the naturally slightly thicker fat in this area and provide a feminine rounded appearance. Arthur Swift and Kent Remington have beautifully described the ideal contour and surface landmarks for identifying the cheek area, based on the mathematical concept of PHI [5]. The techniques utilise a triangle drawn on the face with points at the lateral canthus, ipsilateral oral commisure, and ipsilateral tragus, and drawing an oval with three points contacting the lines of the triangle tangentially. This generally corresponds to an ideal cheek position for soft tissue volumisation in both the male and female face, the significant difference being only the point of greatest projection.
The Nose:
The nose is one of the areas of the face where subtle differences occur between the sexes. There are many angles and measurements to define an ideal nose shape, position and proportion [10], however for the purposes of the sexually diamorphic traits that can be effected, we will discuss two main angles. The nasolabial angle is the angle between a line drawn from the lip border to the base of the collumela, and a line drawn from the base of the collumella to the nasal tip. This angle describes the degree of rotation of the nasal tip. The ideal male angle has been described as 97 degrees and the ideal female angle as 105.9 degrees [11] The same study identifies different preferences in different ethnicities, with native americans and african americans preferring a more acute angle. A similar more acute nasolabial angle preference was found in a study in the asian patient population [12]. It is important to bear in mind therefore the cultural preferences of the patient being treated, the general rule however is that the angle should be more obtuse in a female patient in general, and slightly upturned in a female caucasian. The other angle of significance is the naso-frontal angle. This is the angle of the radix, the lowest point on the nasal bridge and is formed by a line running from the radix to the glabella, and from the radix along the dorsum on the nose. The angle is greater in females than males, one study identifying an average female angle of 138 degrees and a male angle of 130 degrees[13] The postition of the radix is also of importance, in the female it should be at the level of the lash line, in the male it tends to be higher, at the level of the tarsal fold, and more confluent with the glabella. When performing rhinomodulation with toxins or fillers it is important to respect these angles, as beautification does not involve masculinazation of a female feature or vice-versa.
The Jawline and Chin
The consensus of what constitutes an attractive jaw line in both males and females tends to vary with ethnicity[14] and in todays multicultural society the practitioner must not just be aware of the local norms, but also be open to their patients expectations from treatment. The gonial angle is the angle formed by the mandibular line (a line running tangentially to the two lowest points on the anterior and posterior mandible) and the ramus line ( a line running through the two most distal points on the ramus). This angle has been shown to be lower in males than in females.[15] Additionally the male mandible is wider at the gonion, due to eversion of the bone caused by masseteric attachement, and the bulk of a larger masseter muscle. The male chin is larger than a female chin, with a more widely set trigon. The underlying anatomy matches the Hollywood ideal of a male having a wide, sharply defined jaw, sharply angled and with a wide flat chin. The female counterpart has a narrower softer chin, gently sloping from auricle to a narrower more pointed chin. We can employ both masculinasation and feminisation techniques to the jawine and chin, using toxins to narrow down the masseter or curve a chin, and fillers to widen a jawline, increase definition, add a sharper gonial angle or flatten and enlarge a chin.
Perioral area
Perioral rejuvenation is a very common patent request amongst females but not so much in the male population. After appropriate lip rejuvenation there is often not much else required in a male patient, but female patients tend to suffer more from perioral smokers lines, as well as much more severe perioral wrinkling[16] that may require resurfacing treatments in addition to toxins and fillers. The underlying reasons for this difference are not clearly understood, but it is thought to be related to the male skin being thicker and more seborhheic, with thinner underlying fat and a greater vascularity. Interestingly one study has shown that the female obicularis oris attaches 1.5 times closer to the skin in female subjects than in male subjects[17], which provides a reasonable explanation for the greater tenancy to smokers lines in females. Where it would be common to address a perioral female case with toxins, fillers and CO2 pulsed laser a similar approach to the male perioral area may result in feminisation of the skin and should be performed with caution.
Case Studies:
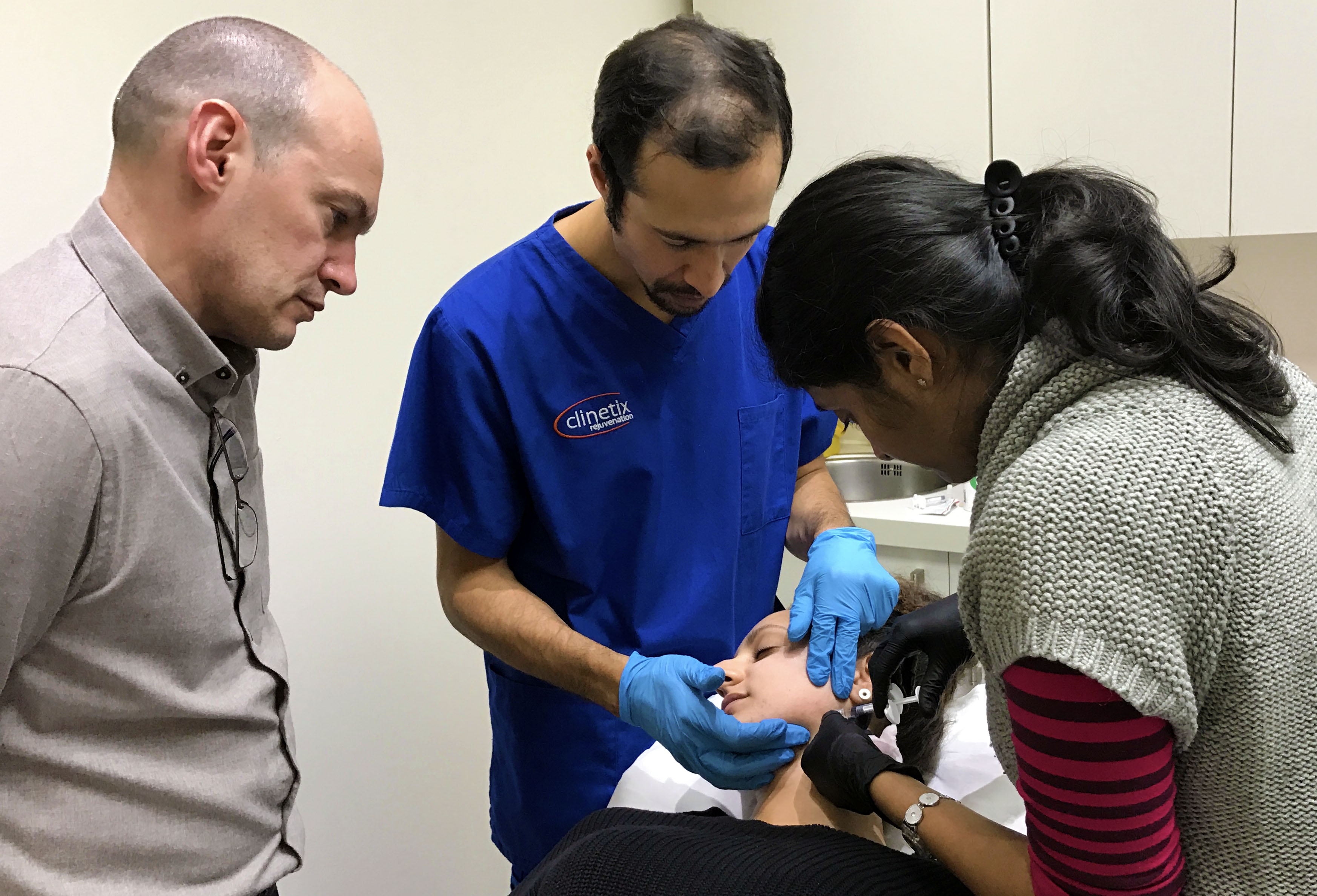
In June 2015 we delivered a live demonstration of the differences in the assessment and injection techniques for male and female rejuvenation at FACE. Our male patient was 40 years old and had previously had mid facial volumisation with Radiesse and upper face toxin treatments 2 years previous. The female patient was 45 years old and had previously had mid facial hyaluronic fillers and upper face toxin more than 2 years previous.
We discussed the outcomes desired by each patient. The male wanted a result that was not obvious to his peers, made him look less tired and younger whilst maintaining his masculine rugged appearance. The female was less specific but wanted to look fresher and more attractive.
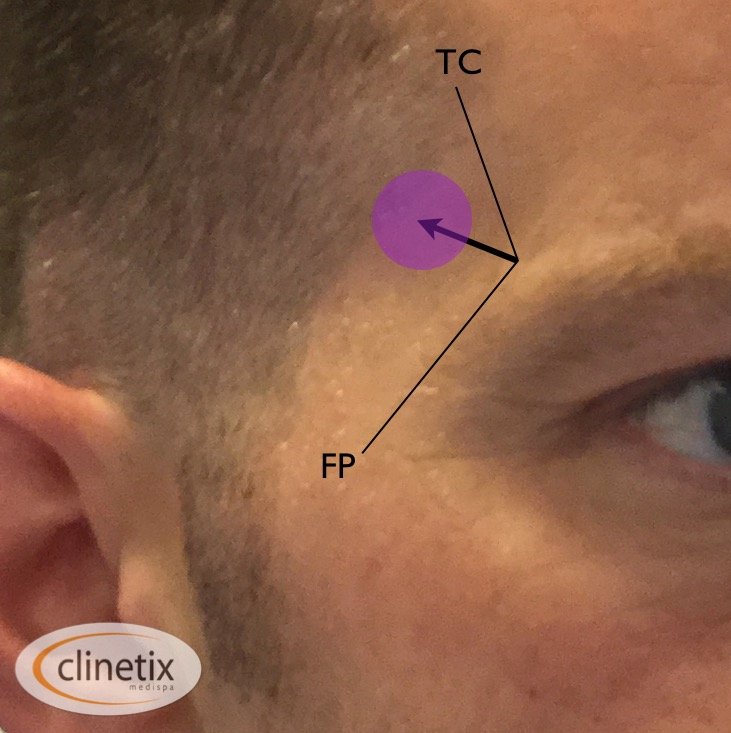
A comprehensive assessment of the male face identified global volume loss, particularly evident at the temples causing an hourglass deformity with loss of the tail of the eyebrow. There was moderate bossing of the central forehead and significant mid facial cheek sagging. The lips where both thinned, and the upper lip inverted causing a lengthening of the philtum. The jawline was fairly strong but had slight softening curve along from the gonion to the chin.(fig 1.) The temple was treated with superperiosteal depots of Belotero Volume, 0.8cc each side placed approximately one centimeter superiolateral to the superiolateral bony rim of the orbit (fig 2.). Further treatments in this area would be repeated at intervals until sufficient revolumsation is achieved. The central forehead bossing was softened but not completely corrected with superperiosteal deposits of Belotero Balance. The cheek was volumised with superperiosteal Volume anteriorly in a single deposit of 0.5 cc with a needle, then a uniform deposition of Volume 0.5cc in the subcutaneous fat of the anterior cheek area using a 25G microcannula. the lips both volumised and the upper lip everted with Belotero Intense 1cc using a 25G cannula and the jaw line was sharpened with subcutaneous threads of Radiesse injected with a 27G needle.
Fig, 3) Male patient immediately after treatment to forehead, temples, lips, cheeks and jawline.Fig. 1) Note the low brow position on a prominent supraorbital ridge with central forehead bossing. the patient also has significant anterior midfacial volume loss with subsequent midfacial ptosis. The upper lip is thin and inverted and the jaw line slightly soft and curved.Fig. 2) TC – Temporal Crest, FP Frontal Process of Zygoma, Purple Dot – Position of Volume placement
For the female patient a full assessment highlighted signs of ageing as a result of loss of volume associated with the temples, checks, jaw, maxilla and chin. The temples we augmented using the same technique as the male with 0.4ml of volume. The female temple remained concave, but helped blend the contour of the forehead smoothly into the lateral cheek prominence. The apex of the cheek is located at the intersection of the alar tragal line and a vertical line dropped vertically from the putter canthus of each eye. A bonus of 0.2 ml of volume was injected supraperiosteally at this point with a 30G 0.5mm needle to widen the bizygomal distance. Small boluses of volume were deposited across the lateral and mid cheek to lift and project the midface. Finally, lateral check contouring was defined as described by Swift and Remmington using a 25G 1.5 inch cannula subcutaneouly, depositing more filler medially. The lower third of the face showed the most marked signs of ageing. Perioral rejuvenation included restructuring the vermillion boarder by injecting Belotero Balance intradermally along the vermillion boarder. The White lip was also injected directly intradermally using a blanching technique described by Patrick Micheels.[18] The chin was injected supraperiosteally with several boluses of standard dilution Radiesse at the pogonion to lengthen and project the chin. Radiesse was also injected in the menton area to reduce the mental crease and smooth the contour between the lower lip and the chin.
Fig. 4) Female model right profile beforeFig. 5) Female model right profile after
Summary:
Aesthetic medicine is still a new and evolving field of medicine. In order to achieve excellence it is not enough to simply keep on top of the evolving products and techniques. If we truly want to acheive excellence we also need to stay ahead of the changing markets. With the increasing number of males presenting for rejuvenation treatments it is imperative that the expert practitioner extends his or her expertise to the matter of male rejuvenation. What constitutes a beautiful female face, and the techniques to non-surgically make a female face beautiful will not translate onto the male patient. An understanding of the different anatomical characteristics as well as the different expectations for treatment will.
Drs Emma and Simon Ravichandran are recognised and respected experts in the aesthetic medicine field who offer a multitude of training courses. To find out more about training courses visit www.clinetixtrainingacademy.co.uk or contact courses@clinetix.co.uk
American Society for Plastic Surgery 2011 statistics. Available from: http://www.plasticsurgery.org/News-and-Resources/2011-Statistics-.html
Snow, C.C, Gatliff, B.P, McWilliams, K.R. Reconstruction of facial features from the skull: An evaluation of it’s usefulness in forensic anthropology. Am. J. Phys. Anthropology. 33:221, 1970.
Douglas K. Ousterhout DDS., M.D Feminization of the forehead: Contour Changing to Improve Female Aesthetics. Plastic and Reconstructive Surgery, Vol 79, No. 5 pp701-711. May 1987
Goldstein S.M, Katowitz J.A, The Male Eyebrow: A Topographic Anatomic Analysis. Ophthalmic Plastic and Reconstructive Surgery Vol 21. No. 4 pp. 285-291
Mendelson B, Wong C. Changes in the Facial Skeleton with Aging: Implications and Clinical Applications in Facial Rejuvenation. Aesthetic Plastic Surgery (2012) 36:753-760
Scheib JE, Gangestad SW, Thornhill R. Facial Attractiveness, symmetry and cues of good genes. Proc Biol Sci 199; 266(1431):1913-1917
Wysong A, Kim D, Joseph T, MacFarlane DF, Tang JY, Gladstone HB. Quantifying soft tissue loss in the aging male face using magnetic resonance imaging. Dermatol Surg, 2014;40(7):786-793
Wysong A, Kim D, Joseph T, Tang JY, Gladstone HB. Quantifying soft tissue loss in facial aging; a study in women using magnetic resonance imaging. Dermatol Surg, 2013;39(12):1895-1902
Prendergast, PM. (2012). Facial Proportions. In: A. Erian and M.A Shiffman Advanced Surgical Facial Rejuvenation. Berlin: Springer-Verlag. p15-21.
Sino HH, Markarian MK, Ibrahim AM, Lin SJ. The ideal nasolabial angle in rhinoplasty: a preference analysis of the gneral population.
Choi J Y; Park JH; Hedyeh J, Sykes JM. Effect of Various Facial Angles and Measurements on the Ideal Position of the Nasal Tip in the Asian Patient Population. JAMA Facial Plast Surg. 2013;15(6):417-421
Ferdousi M A, Mamun AA, Banu L A, Paul S. Angular Photogrammetric Analysis of the Facial Profile of the Adult Bangladeshi Garo. Advances in Anthropology 20134 Vol.3, No.4, 188-192
Kane M A. “Is there a double standard of beauty”? Or can common/ general beauty be applied to Asian and Caucasian Patients?” World Congress of Dermatology, Seoul, Korea, May 27, 2011.
Chole HC, Patil RN, Chole SB, Gondivkar S, Gadbail A, Yuwanati MB, Association of Mandible Anatomy with Age, Gender and Dental Status: A Radiographic Study. ISRN Radiology Volume 2013 Article ID 453764
Wojnarowska F. Clinical aspects of ageing skin. In Fry L. editor. Skin problems in the elderly, 2nd Ed. Edinburgh: Churchill Livingstone: 1985, pp28-46
Paes EC, Hans J, Teepen M, Koop W A, Kon M. Perioral Wrinkles: Histologic Differences between Men and Women. Aesthetic Surgery Journal Vol 29(6) 2009 pp467-472
Micheels P, Sarazin D, Besse S, Sundaram H, Flynn TC. A Blanching Technique for Intradermal Injection of the Hyaluronic Acid Belotero, Plastic and Reconstructive Surgery Vol 132, No. 4S-2 pp59-68
Dermal Fillers For Dark Circles Under The Eye?
3rd September 2016 | Dermal Fillers
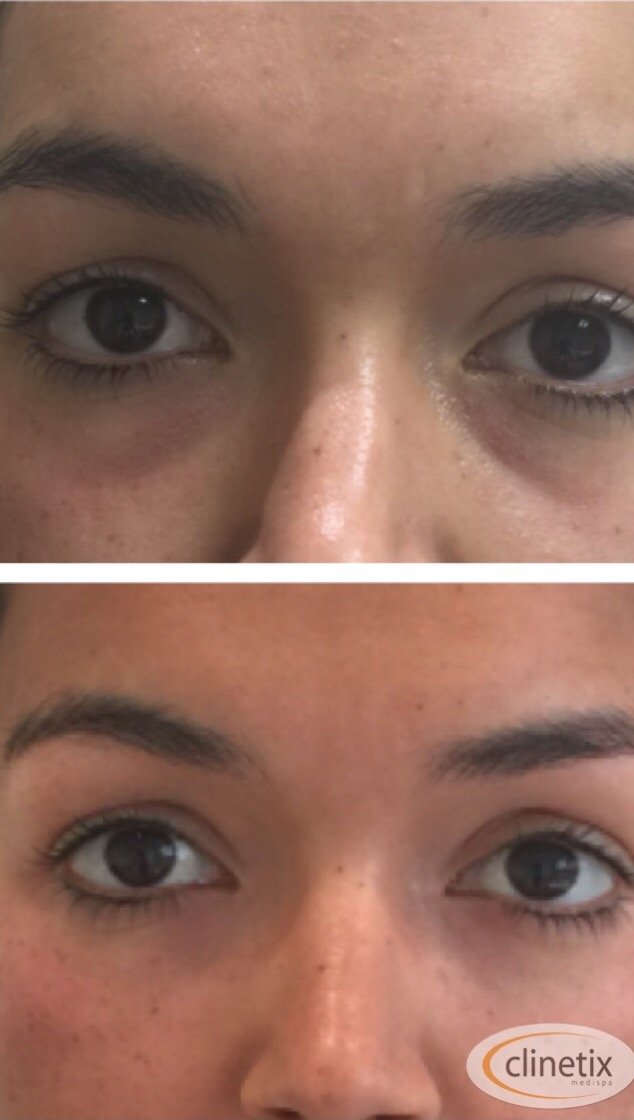
Having dark circles under the eye can be distressing for many people. They can give the appearance of looking tired, unwell or run down.
What are the dark circles?
In many cases the appearance is caused by shadow, rather than a darkness to the skin itself. There is a natural anatomical hollow underneath the eye that can sometimes just be a bit more pronounced as a result of your genetics. It also tends to develop with age and appear more prominent as fat under the skin thins and sags. The problem is the light reflecting on the skin around the area but not of the hollow itself, but not in the hollow itself. This is sometimes called the tear trough or a tear trough deformity.
Other causes of dark circles such as skin irritation, allergies and pigmentation are not suitable for treatment with dermal fillers but our doctors will be able to identify this at your consultation and advise you as to the best treatment.
So, so long as your dark circles are caused by hollowing under the eye, they can be treated with dermal fillers.
How do dermal fillers in the tear trough work?
Using dermal fillers in this area is part of a “peri-orbital” rejuvenation. Which means rejuvenation around the eye area. Firstly the exact cause needs to be identified by a thorough assessment, as there are a few different causes for the hollowness. Once the correct areas have been identified a dermal filler gel is injected extremely carefully in the right amounts into the right areas. It is usual for more than one type of filler to be used, as we need to replace volume in different anatomical zones.
After injection there is an immediate plumping and smoothing of the area and reduction in the dark circle appearance.
How many treatments are needed?
The area under the eye is particularly delicate and because of this it is often recommended to have treatment with dermal fillers done over a couple of sessions. This helps reduce the possibility of complications such as bruising and swelling.
Is it safe?
The area around the eye is delicate and the anatomy is very complex. Correction with dermal fillers requires the correct amount of the correct sort of filler to be placed very precisely in order to get the best result. If the filler is injected into the wrong area, or if the wrong sort of filler is used it is possible to see lumps or swellings through the skin, and sometimes you can have bruising or prolonged swelling and fluid retention under the eye. Because of this it is important that your treatment is performed by someone who has expertise in dermal fillers specifically in this area.
How is the treatment performed?
Once it has been decided that you are suitable for treatment, a thorough examination will show the areas that require to be injected for a natural result and your practitioner will explain the treatment plan. The treatment does not usually require any anaesthetic as the needles that are used are typically very small and the fillers themselves often have a small amount of anaesthetic within them. The fillers can be placed using a few different techniques. Tiny needles can be used that allow precise placement of dermal filler in specific areas, and cannula can be used to spread fillers out more evenly in other tissue planes. Often a combination of techniques will get the best results.
There is no downtime and you can leave the clinic shortly after the treatment and carry on with your normal activities.
What happens after treatment?
There may be a small amount of bruising or swelling. If this occurs it will usually settle down in a few days. Your practitioner will be able give you individual advice on what you can do to help minimise any bruising or swelling following dermal filler treatments.
Clinetix arrange a two week follow up appointment following treatment to assess the improvement and make sure there are no complications. It is important that you keep this appointment as it allows us to keep track of your treatments and your response to treatments.
If you are concerned about the appearance of dark circles and would like a consultation with one of our medical team to discuss your treatment options please feel free to get in touch.
You can book a consultation with any of our team by calling the Hyndland Clinic on 01412210229 or the Bothwell Clinic on 01698854221. Alternatively you can contact us here on our contact page.
This website uses cookies to improve your experience. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checkbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checkbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
 Nasolabial Folds are the lines that run from the corner of the nose to the corner of the mouth, and marionette lines are the lines that run from the corners of the mouth down to the chin. People often notice them as being the first visible signs of an ageing face and often present to an aesthetic clinic to have them corrected with injections of dermal filler.
Nasolabial Folds are the lines that run from the corner of the nose to the corner of the mouth, and marionette lines are the lines that run from the corners of the mouth down to the chin. People often notice them as being the first visible signs of an ageing face and often present to an aesthetic clinic to have them corrected with injections of dermal filler.








{kind=link}