Unwanted body hair has long been an aesthetic concern for both men and women, with evidence having been found for recipes for hair removal compounds dating as far back as 3000BC! Some modern commentators feel that the proliferation of female nudes in art since the sixteenth century has encouraged the idea that the female form should be hairless. The modern form of this is obviously the mass media exposure everyone not living in a cave is bombarded with through magazines, social media, TV and film. Whatever the causes this is a cultural and fashionable concern that doesn’t seem set to go away in out lifetimes.

So we agree that the desire to have smooth hairless skin is something deep seated in our cultural psyche, and you have decided that you are amongst the majority of people willing and happy to follow the trend. You are familiar with the current accepted methods of hair removal such as waxing, shaving or epilation but are getting fed up with the time involved, the discomfort and the frequency of treatments required. You’ve heard about laser hair removal, some people have told you it’s painless and lasts for ever, and others have told you it’s agony and ineffective! What’s the truth?
How does the treatment work?
“Watch the video here”
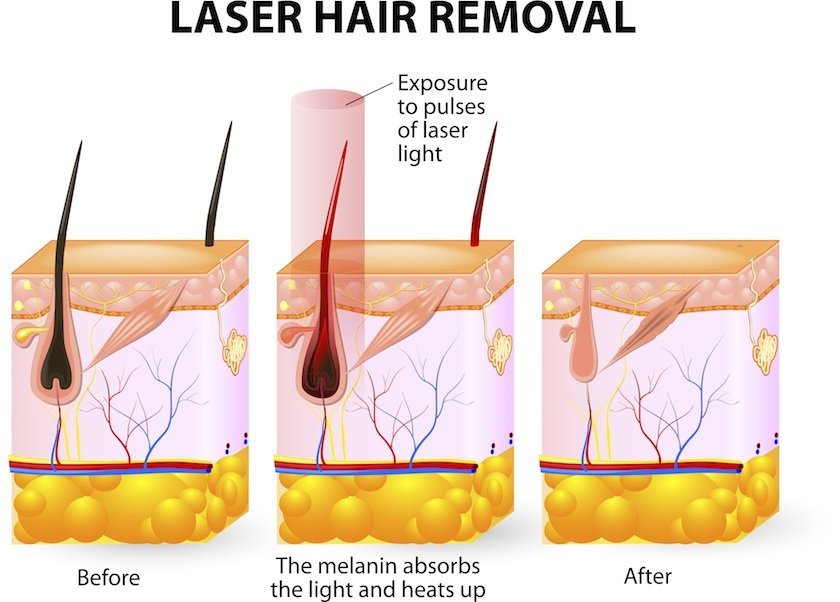
The reason your hair grows back after most forms of hair removal is that you only remove it at the level of the surface of the skin. The hair follicle itself actually extends quite deeply into the skin to a structure called the hair “bulb”. This bulb will constantly regenerate the hair follicle causing return of growth within a relatively short time, Just think of how often some men need to shave their beards to keep a smooth chin!
The goal of semi permanent hair removal is to remove the bulb itself, thus preventing future regrowth. Both laser and IPL treatments do this using light energy. You will know how light energy heats things up, think of how hot the buckle on your seatbelt can get in your car on a hot day. What the Laser and IPL devices do is apply a specific part of the light energy to the skin, that is preferentially absorbed by the pigment in the hair. This energy converts to heat along the entire length of the hair shaft causing it’s instant destruction. When the shaft of the hair is in contact with the bulb of the hair the bulb also gets destroyed, and can no longer produce new hair. It’s as simple as that!
Why do you call it Semi Permanent?
Good point. You would think that when the hair follicle is destroyed that should be the end of it for ever. Unfortunately that isn’t the case. Your skin has an ability to create new hair follicles as time goes on, meaning the hair will very slowly recover.
I’ve heard I need several treatments? Shouldn’t it work with just one?
Won’t work with just one I’m afraid. The reason for this related to the way it actually works. We’ve mentioned it destroys the hair bulbs in contact with the hair shaft, and that’s the problem. Not all hair shafts are actually in contact with a working shaft, they tend to lift off and float towards the surface as they mature. As a rule only one quarter of the hair gets treated in any one session. This means that between 4 and 6 sessions are often required, between 2 and 4 weeks apart.
Am I suitable for treatment? I’ve been told before that I have the wrong skin type.
Most people are suitable for treatment, the decision is made based upon the skin colour and the hair colour. Because the technology depends on the pigment in the hair follicle, the darker the hair the better. Completely white hair is very difficult to treat this way, the lighter the hair colour the more treatment sessions are required. When considering the skin, we want the energy to be absorbed by the pigment in the hair follicles, not the pigment in the skin, so we have to change the energy levels in darker skin types, so dark skin types may also require more sessions to get a good result. So to summarise pretty much anyone can get treatment, it’s just that the number of treatments required and the overall result will differ for light hair and for darker skin.
How many treatments are required, and how long do the results last for?
For most people a course of six treatments is recommended. This is usually effective. Due to the regeneration of your skins hair follicles, smaller hairs tend to appear very slowly after treatment and a single session is recommended once every year or so to keep them at bay.
Is the treatment painful?
Not at all. Older technologies using straightforward light energy alone were quite uncomfortable, but modern devices use other technologies together that reduce the overall energy required, and cooling to reduce the sensation.
I’d like to give it a try. What else do I need to know?
If you’ve read this far and you are interested in finding out more or booking a treatment session there are a few things you should know. You can’t have treatment if you currently have a tan in your skin, as it may cause burning to the treated area. You also need to avoid sun exposure during the course of the treatment so a factor 50 spf is recommended to be used daily on sun exposed areas. This is a medical treatment and whilst usually safe there is an element of risk. The risk in relation to this treatment is the small chance of blistering, redness and burning of the skin. To make sure this doesn’t happen a full assessment of your skin type is made, so the safest settings are programmed into the device. We also require that you have a patch test of the treatment at the chosen settings at least 24 hrs before your treatment, so we can assess the response.
If you would like more information you can contact us by phone, on 0141221029 or e-mail us here