Clinetix Medical Practitioner Dr Caroline McAuley BDS.MJDF Dip Rest Dent RCS recently wrote an article for Aesthetics Journal on how to the clinical skills she learnt from her dental training relate to aesthetic medicine. This article is aimed mainly at medical aesthetic practitioners but we hope that you find it interesting if you read to the end.
Applying Skills from Dentistry to Aesthetics
Dr Caroline McCauley explains how the clinical skills learnt from dental training relate to aesthetic medicine and provides tips for a successful transition.
Aesthetic medicine is a speciality with ever-increasing popularity, requiring an underpinning medical knowledge to provide safe and effective treatments, as well as extensive training and investment in continued professional development and learning.
Soft skills, as well as academic knowledge, are essential in aesthetic medicine to achieve excellence as a practitioner in a competitive market.
Beginning my training in aesthetic medicine after completing a Diploma in Restorative Dentistry and a Certificate in Aesthetic and Restorative Dentistry, I was naturally anxious at the thought of carrying out injectable procedures such as dermal fillers and botulinum toxin. Although dentistry was my comfort zone and it wasn’t easy to be a beginner again, I quickly found that facial aesthetics was, in many ways, like dentistry. As an undergraduate, I had studied head and neck anatomy in-depth and as I learn the basics of aesthetic medicine I realised I had been honing my skills to become an aesthetic medical practitioner since day one of dental school. This article will reassure dental professionals of their place in aesthetic medicine, as well as provide some useful tips for a successful transition.
Consulting patients
Consultation skills are similar in both aesthetics and dentistry, as briefly outlines in Figure 1. Dental postgraduate training has a strong focus on information gathering in a methodical way. Dental students are taught to take a full history, carry out a thorough examination and formulate a diagnosis and treatment plan before they can perform the treatment. Aesthetic medicine is no different, especially in complex cases where the need for a methodical approach is paramount. This begins with taking a thorough history including previous aesthetic treatments, current skincare regimes, and the patient’s hopes and expectations. Then we must carry out an examination – it’s common practice in both dentistry and aesthetics to work in a methodical fashion when carrying this out. For example, in dentistry we assess the extraoral skeletal form and then, intraorally, the teeth and soft tissues. In aesthetics we should be equally as methodical, assessing horizontal thirds from the upper to the lower face and in the vertical plane from the outside in. This process can be time consuming, however ensures that just like in dentistry, we do not miss key information.
| History taking | Medical / social / previous treatments / wishes and aspirations |
| Examination | Methodical approach – upper third to lower third/ skeletal pattern/ skin/ photodamage/ volumetric changes/ asymmetries |
| Information gathering | Clinical photos – full face/ 90 degrees/ 45 degrees. Lips – full smile/half-smile |
| Treatment planning | Treatment planning/options discussion – having a full set of clinical photos can allow you to treatment plan with your mentor |
| Estimates/ budget | Treatment can be phased depending on the patient’s budget. Estimates signed/emailed to patient |
| Consent forms | Discussed/ signed and emailed to the patient |
If we take time in both disciplines to discuss diagnoses and treatment options with our patients, we are allowing our patients time to understand the options, acting in their best interests and allowing them to consent to any treatments in a meaningful way.
Practising in an ethical manner is of the utmost importance in both fields. The General Dental Council (GDC) is the UK regulatory body which all UK dentists must be registered with. It lists non-surgical cosmetic procedures as an extended duty of dentistry, and therefore it is essential to follow the guidance set out by the GDC in its Standards for the Dental Team (1) document when treating aesthetics patients. This document emphasises the need to practice the core principles outlined above; putting patients’ interests first, communicating effectively with them and obtaining valid consent.
Communication
In the various medical roles, we learn early on the importance of developing our ‘soft skills’. They enable us to communicate effectively with our patients, to make them feel at ease and trust in our ability to look after their needs. Traditionally, dentistry can be an anxiety-inducing for patients and one of my goals as a dentist is to dispel that fear and anxiety. I have always taken time to build rapport with my patients, striking a balance between friendly and approachable, yet maintaining a professional and knowledgeable approach. It is as important in aesthetic medicine to build a business that ensures that the patients we work so hard to get into our clinic with digital marketing, patient referrals and the like, keep returning for their treatments. Building good relations with patients makes day-to-day work more enjoyable and is advantageous if there is an undesirable outcome following treatment. Patients are more likely to be forgiving should this occur if you have invested in building a relationship with them.
A piece of advice that has stuck with me was given to me on a postgraduate aesthetic dentistry course. This was to look in the mirror and practice saying, “The cost of that treatment will be £2,000”. This was said rather flippantly but the sentiment holds true. Talking about money is an essential part of the general dental practice business model and I have taken into my aesthetic practice with ease. Many medical professionals who transition into aesthetic medicine are not used to money changing hands or discussing costs with their patients and can find the subject difficult to broach. However, talking about the cost of treatments without embarrassment is an essential skill to master. In my experience, patients have already researched the prices of your clinic and are prepared to pay for aesthetic treatments, far more so than in dentistry as usually, it is treatments they ‘want’ rather than ‘need’.
Anatomical knowledge
In undergraduate training, medical, dental and nursing students spend a significant portion of their degree studying head and neck anatomy – the blood vessels, the nerve innervations, the facial musculature and skeletal development. This knowledge is invaluable to help assess a patient’s facial shape and bone structure to understand if there is any deviation from the normal pattern and, if so, how we could potentially correct and camouflage this using dermal fillers. While aesthetics may focus on reversing the signs of ageing, environmental damage or enhancing a patient’s features, it can also be valuable in offering a non-surgical alternative for skeletal or muscular deviations from normal. In-depth knowledge of the blood and nerve supply of the face is incredibly important to allow practitioners to undertake treatment safely and avoid complications.
Transferrable treatments
There are many treatments performed by aesthetic professionals which are related to dentistry. The knowledge gained about facial muscles during undergraduate dental training is there, ready to tap into achieve desired results for our patients’ treatments and practice safely.
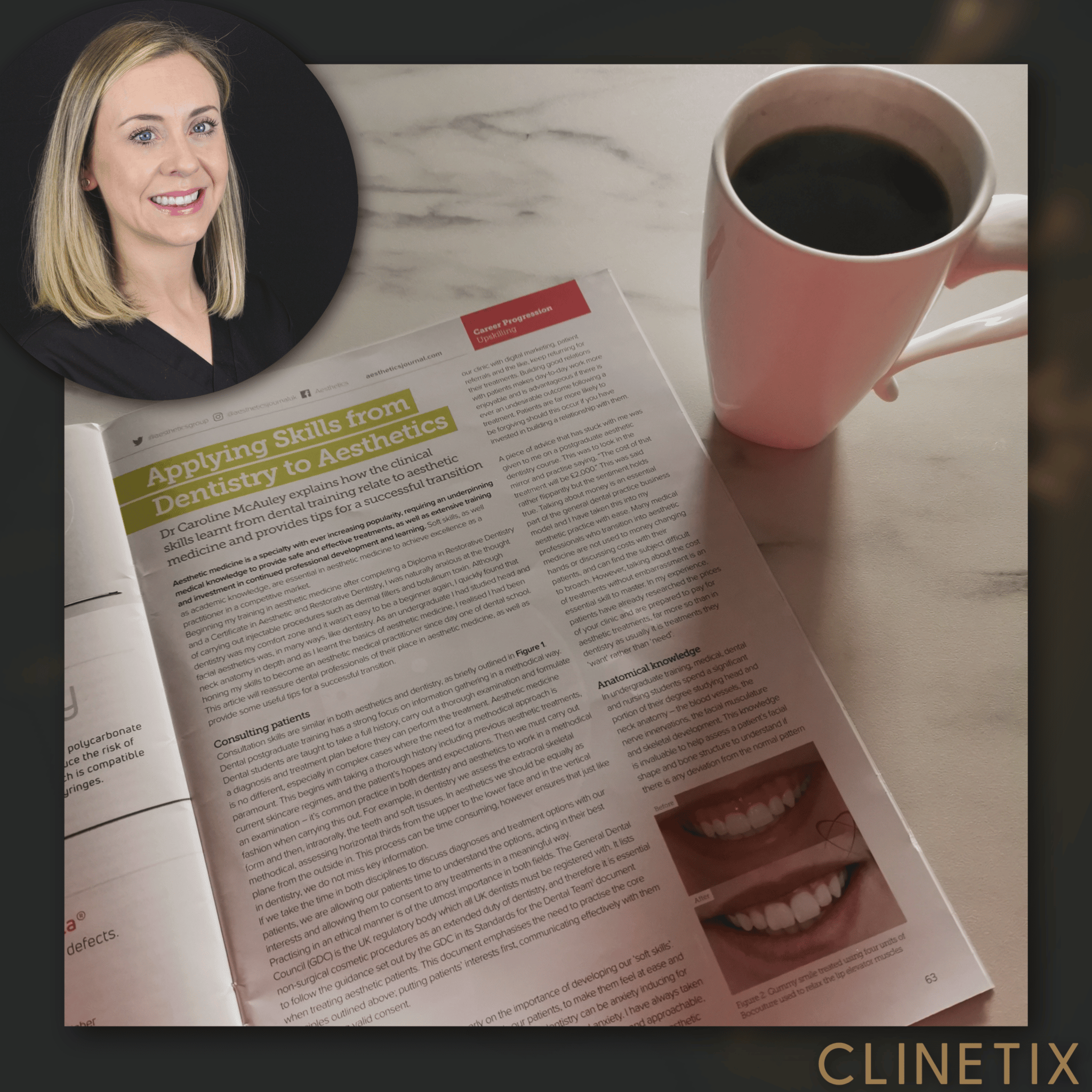
During my time in dental practice I have had numerous cases where a patient presents complaining of a ‘gummy smile’, referring to an excess amount of gum on show. Before moving into aesthetics, I treated this problem with crown lengthening surgery. However, a contributing factor to a gummy smile is a hyperactivity of the muscles which elevate the upper lip.
A small amount of botulinum toxin can relax these muscles while also achieving an aesthetically pleasing outcome for the patient (Figure 2) (2,3). In my experience, this is a far less invasive treatment and could potentially avoid the need for a complex dental procedure so it can be a good alternative.

Figure 3 shows a patient who attended our clinic as she was unhappy with the appearance of her chin and jaw. The treatment that had been suggested prior to her presenting at our clinic was to undergo orthognathic surgery, in order to reposition her lower jaw forward into a ‘correct’ alignment. However, this patient had no functional issues and ehr concern was solely cosmetic, meaning she wanted a less invasive approach. Dentists will routinely carry our an extraoral examination of a patient’s skeletal form as part of a full examination. Deviation from a ‘normal’ skeletal pattern can result in functional jaw issues and a displeasing appearance. Having the knowledge to assess the skeletal form can enable the aesthetic practitioner to use dermal filler to correct and enhance a patient’s skeletal profile. In this case, dermal filler was used to enhance the appearance of her chin and jawline, camouflaging the appearance of her retrognathic mandible.
Tips for future success
For me, my success moving from dentistry to aesthetic medicine has come down to continued support. I am fortunate to work in a clinic that is run by two fantastic aesthetic medical practitioners who are always there to answer my questions and give advice. Having the support of like-minded colleagues has made the transition easier as I always have someone to go to for help and advice and it has allowed me to expand my field of practice and grow in confidence in exploring new treatments.
Finding a mentor, whether it be a colleague who is more experienced in aesthetic treatments or a teacher on an aesthetic course you have subscribed to, can help answer questions, troubleshoot problems and lend an ear to any issues you may be experiencing. Just as I have in my dental career, furthering your education with webinars, advancing skills courses and conferences is essential to keep up to advance your knowledge and skills in the rapidly progressing world of aesthetic medicine.
Another tip for transitioning into aesthetics is one that was given to me when I graduated as a dentist – don’t try to be too fast. Focus on doing an excellent job and over time your speed will pick up naturally. Trying to work quickly to improve your profit margins will only allow mistakes to creep in, whereas taking your time will allow you to build a portfolio of treatment photographs, reduce stress and fewer mistakes will be made.
The next stage of your career
For dentists entering the field of aesthetic medicine, as well as nurses and doctors, I appreciate it can be overwhelming. Like me, you may feel anxious at the thought of being a beginner again. However, if you take a step back, you will realise that many of the skills required to become a successful practitioner are already there from your undergraduate and postgraduate training, as well as work experience. It takes time to and dedication to learn this new skill, but through seeking the right mentros. and drawing on your previous experience, you will find success in your new endeavour.
Dr Caroline McAuley qualified as a dental surgeon from the University of Glasgow in 2007. She has spent her time working primarily in private dental practice, developing a keen eye for carrying out aesthetic treatments. She has completed extensive training in facial aesthetics at the Aesthetic Training Academy and joined Clinetix in 2019, currently splitting her time between there and general dental practice.
References:
- Standards for the Dental Team, General Dental Council, September 2013
- Polo, M. 2008. Botulinum toxin type A for the neuromuscular correction of excessive gingival display on smiling (gummy smile), American Journal of Orthodontics and Dentofacial Orthopedics 133:195-203.
- Ravichandran, S Ravichandran, E (2017) Essential Summary of Medical Injectable Techniques, Spotlight Editorial.