Dr Emma Ravichandran BDS.MFDS joined a panel of practitioners to share her top tips for successful rejuvenation of the perioral area with Aesthetics Journal.
Treating the Perioral Area
Aesthetics speaks to a panel of practitioners (Dr Jonquille Chantrey[JC], Jackie Partridge[JP], Dr Dev Patel[DP] & Dr Emma Ravichandran[ER]) who share their top tips for successful rejuvenation of the perioral region.
How does the perioral area age?
ER – There are multiple factors involved: there is the intrinsic ageing that we all go through, leading to loss of collagen, hyaluronic acid (HA) and decreased tone in the skin. The underlying muscle, which is predominantly the orbicularis oris, is going to slightly lose its tone and tightness contributing to loss of elasticity in the underlying tissues. You get loss of subcutaneous fat as well; again you lose that plumpness and support to the skin and as people age, there is a decrease in the bony support. There are also extrinsic factors, so if people smoke, have a lot of UV exposure or use sunbeds, that really accelerates the ageing of the skin. (1,2,3).
JP – The perioral area has some of its own issues. The mandible itself is thinning with the ageing process, the density of the bone isn’t what it was in youth and that is going to have an impact on bony support for the mandibular and perioral area. The bone supporting the teeth is also regressing, the teeth are becoming more unstable and you also may have tooth loss, which means that the structural support is missing. The way I explain ageing to my patients is that if you think of the structural bone support as a table and the skin as a tablecloth, the table is getting smaller and the tablecloth then doesn’t have the support underneath it to look as nice as it once did. (1,2,3).
What are the key patient groups seeking treatment for the perioral area?
DP-Mainly women who are middle-aged and older. I’d say the 40+ age group and particularly those in their 50s and 60s. For line around the perioral area, it is weighted towards smokers and those who have a history of smoking – but there are also some who have deep static lines in the area and don’t have a history of smoking.
JC –My most common demographic is 40+, but for young people in the perioral area, I actually perform a lot of corrects. So many people are doing these treatments now and some aren’t doing it very well. Sometimes patients come in with an uneven lip, lumps and a heaviness and over-protrusion, created when the vermillion border is over-injected.
What concerns do your patients often present with in the perioral area?
JC – Three things; firstly the associated buccal far descent that is creating the marionette fold, the second is the perioral lip lines – created mostly in expression when pursing the lips through expression of the orbicularis oris, and the third would be patients wanting gentle enhancement.
ER – Most of my patients will complain of an aged, sad look to the perioral area, such as down-turned corners of the mouth, the nasolabial folds, the marionette area; they will also complain of thinning of the lips and barcode lines or smoker’s lines.
In your opinion, what are the key considerations that must be made when assessing and treating the perioral area?
JC – Do a proper assessment and anatomical diagnosis. Practitioners need to be aware of the dental profile and arcade, the relationship of the teeth, the lips to the nose and the chin. They need to be looking at the looking at the patient from both the frontal and profile view.
JP – Less is more! I think doing smaller treatment modalities but more of them is going to give a better and sager aesthetic outcome. You will have less risk of vascular compression if you aren’t using so much product.
DP – Don’t just look at the perioral area – see it as part of the whole face as, often, particularly in this area, it has become such a focus in the patient’s eyes that is is easy to zoom in and focus on this with them. We have a lot of options for this area, find a nice treatment combination, which is appropriate for that person, based on their wishes and what their expectations are.
How do you approach patients with the following indications?
Loss of volume in the lips
JP – The lips thin as we age. Patients often report that their top lip completely disappears when they do a big smile, so to address this, it is important that we don’t lose symmetry; the top lip to bottom lip should be 1:1:6 ratio. I would use Restylane Kysse, as it’s a cohesive product but also has projection.
JC – It depends on what the patient is trying to achieve, their own perceptions of the proportions and their profile. I look at the patient in expression – kissing, smiling. If they need an increase in their lip height then I’ll consider treating the vermillion border; if they have a flatter cupid’s bow, then I’d inject that; and if it’s just a general lip fullness that they requests I would inject the pink body of the lip. I’d use Juvederm Ultra Smile or Volbella in the perioral area because they are very cohesive.
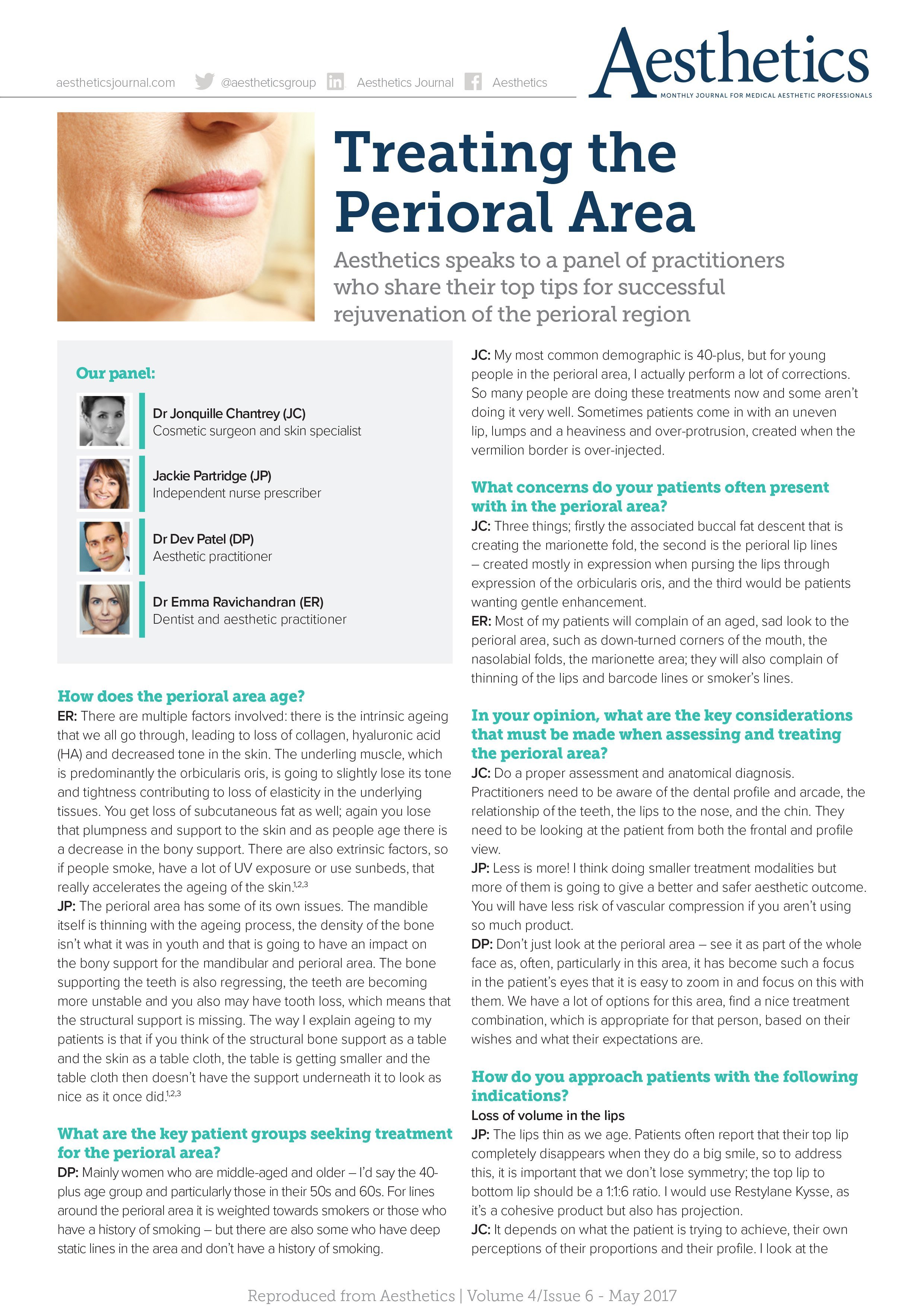
ER- You are assessing the relationship of the mandible and the maxilla – consider the symmetry and proportions of the lip with respect to the face and be cautious of the patient’s profile. To replace the loss of true volume within the vermillion, I will use Belotero Intense and a 25G 1.5-inch cannula and will insert the product in the subcutaneous plain, which is the safest way of injecting the product subcutaneously with regards to the risk of injecting the superior labial artery.
Lines and wrinkles or ‘smoker’s lines’ around the mouth
ER – You need to know what has caused the lines and make a proper diagnosis to determine whether they have just genetically inherited the lines, whether they smoked or continue to smoke, use vaporisers, or are real sun worshippers, which will all encourage perioral lines to form. If they currently do, they are not good candidates for treatment.
JC – It depends on the underlying diagnosis, some patients need support around the vermillion border to get good results; I’d do a small injection into the vermillion border to support that. If it’s just early lines, I’d get the patients to express and purse their lips and do microinjections into the line itself with Juvederm Ultra 2 or Volbella.
DP – There are lots of options depending on the severity. If it’s very early and there are a lot of dynamic lines then botulinum toxin A may prevent them from forming. I also might use the Needle Shaping/ Vibrance device, which triggers collagenases and production of elastic fibres and will give subtle improvement to those early lines. Once they have static lines, if they want a quick fix, I’d use the blanching technique with Belotero Soft. Skin resurfacing by remodelling the skin would give them a longer improvement and the type would depend on the patient. My options are fractitional ablative laser, I use iPixel; vertical microneedling such as Dermapen, or peels – I use Enerpeel MA because they have a specific peel for the perioral area. Soft surgery is also an option – Plexr is good for working on the deep static lines that are already there, you use it by treating the area immediately adjacent to the line and one or two treatments will give you really good results.
Nasolabial Folds
JP – We are moving more away from treating the individual nasolabial folds and instead we are augmenting areas to give you lift in the mid-face, which again will correct areas of volume loss further down the face without adding weight to the lower face.
ER – You need to know what’s cause the nasolabial fold – the nasolabial fat compartment is probably the last fat compartment to lose fat in the face and most of the descent comes from loss of the mid and lateral cheek fat compartments to they need to be addressed first. We also get widening of the nasal aperture as we age, loss of bone, a widening of the nose and deepening in the alar triangle. Often, it’s the shadow in the triangle that gives the impression that the nasolabial line is bigger than it is. If we lift and push that triangle forward with a bolus of filler we reduce the shadow, impacting on that depth or the apparent depth of the nasolabial fold.
The Marionette Area
JC – Most patients presenting with a marionette fold usually have some degree of descent in the mid-face – so assess the mid-face and see if it needs treating, adopting an indirect approach to treatment. If the patient wants a direct approach, I tell them the results won’t be as good, but I will treat the marionette fold directly.
DP – My approach would be to use a simple HA filler – Belotero Volume or Intense – and I would put it in and around the problem areas and follow the principals of not just filling a line, and certainly not just filling a fold, but replacing the support around the area giving them a lift.
ER – It’s important to have adequate support for the lower and upper lip and ensure that there is a nice blend from the cheek into the chin area – you don’t want to overfill. Choose the right produt that has the right level of elasticity, plasticity and cohesiveness so that it doesn’t migrate and will move on animation. You want to place it subcutaneously using a cannula to minimise the risk of bruising – it’s about pushing the marionette area forward so there is a nice colour refraction.
Improving Skin Texture and Overall Apearance at the clinic
JC – It starts with a diagnosis and medical history, followed by an assessment. Is the skin dehydrated, oily, rough and dull? Is there increased pore size? in office, I love Juvederm Volite because we can improve skin texture, elasticity and hydration with a single session. I also use different strengths of TCA chemical peels for skin texture improvement. I find that they offer an enhanced smoothness that is difficult to achieve with other modalities.
JP – I might consider a laser peel for rejuvenating the skin to stimulate collagen production and tightening pore size; it’s important that we utilise different modalities for treatment because there are so many treatment options which work in harmony to give the best outcome. You can also consider Restylane Skin Boosters to add hydration in the area of concern for patients, to give an improvement around the perioral area, especially for acne scarring as we know the chin especially can be affected.
DP – I find chemical peel and fractional ablative laser treatments give very minimal downtime of two to three days. They have really fantastic results, addressing skin texture, pigmentation and even some of the vascular changes you get with ageing and sun damge.
Improve overall appearance using home care
ER – Before other treatments like IPL, laser or peels, I would get the patient onto a good skin health programme for about two to four weeks. We would then introduce maybe a combination of either hydroquinone product, a non-hydroquinone products or a retinol product, in order to even the texture and to try to imporve any pigmentation.
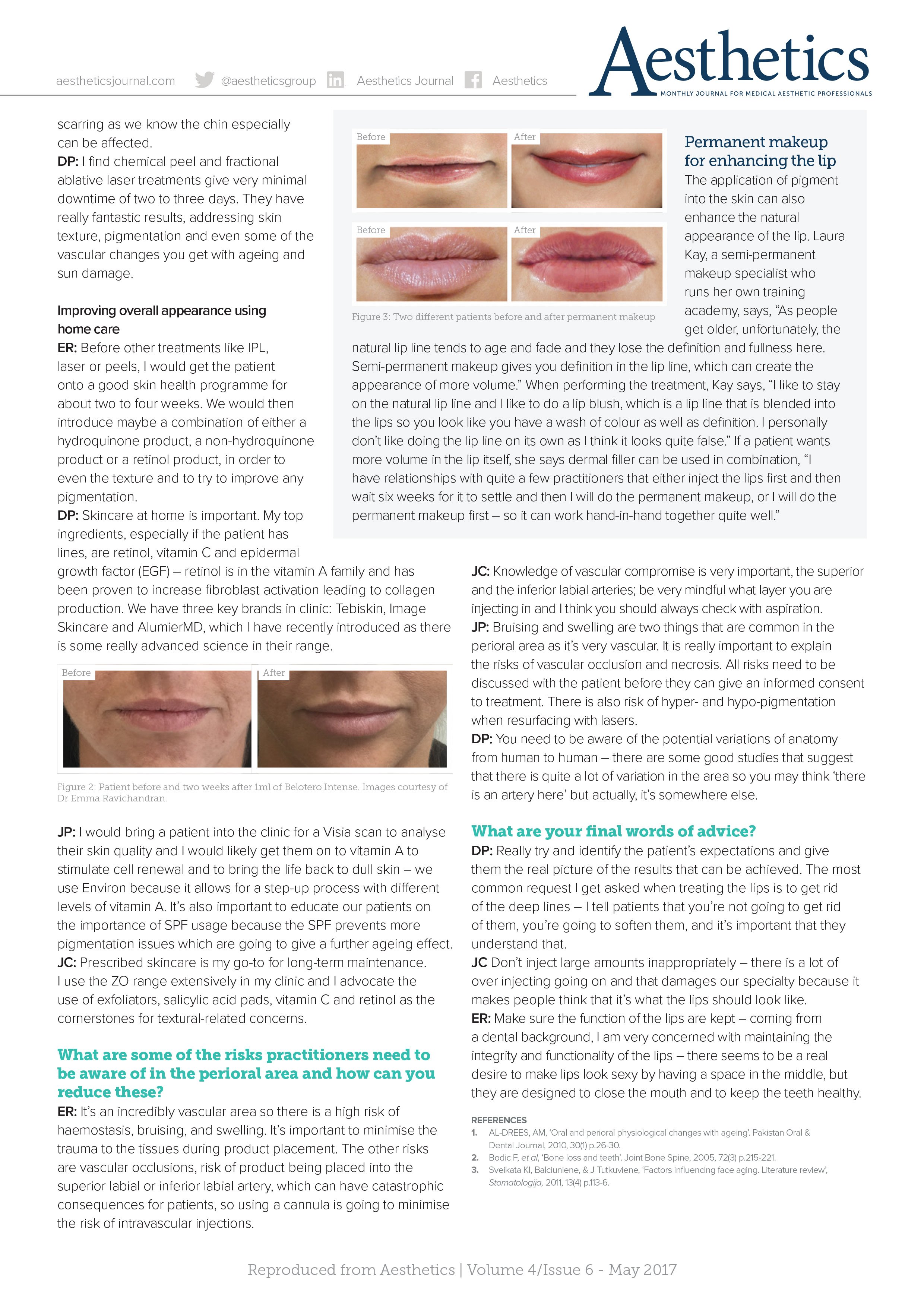
DP – Skincare at home is important. My top ingredients, especially if the patient has lines, are retinol, vitamin C and epidermal growth factor (EGF) – retinol is in the vitamin A family and has been proven to increase fibroblast activation leading to collagen production. We have three key brands in clinic: Tebiskin, Image Skincare and AlumierMD, which I have recently introduced as there is some really advanced science in their range.
JP – I would bring a patient into the clinic for a Visia scan to analyse their skin quality and I would likely get them on to a Vitamin A to stimulate cell renewal and to bring the life back to dull skin – we use Environ because it allows for a step-up process with different levels of vitamin A. It’s also important to educate our patients on the importance of SPF usage because the SPF prevents more pigmentation issues which are going to give a further ageing effect.
JC – Prescribed skincare is my go-to for long-term maintenance. I use the ZO range extensively in my clinic and I advocate the use of exfoliators, salicylic acid pads, vitamin C and retinol as the cornerstones for textural-related concerns.
What are some of the risks practitioners need to be aware of in the perioral area and how can you reduce these?
ER – It’s an incredibly vascular area so there is a high risk of haemostasis, bruising, and swelling. It’s important to minimise the trauma to the tissues during product placement. The other risks are vascular occlusions, risk of product being placed into the superior labial or inferior labial artery, which can have catastrophic consequences for patients, so using a cannula is going to minimise the risk of intravascular injections.
JC – Knowledge of vascular compromise is very important, the superior and the inferior labial arteries; be very mindful what layer you are injecting in and I think you should always check with aspiration.
JP – Bruising and swelling are two things that are common in the perioral area as it’s very vascular. It is really important to explain the risks of vascular occlusion and necrosis. All risks need to be discussed with the patient before they can give an informed consent to treatment. There is also a risk of hyper- and hypo-pigmentation when resurfacing with lasers.
DP – You need to be aware of the potential variations of anatomy from human to human – there are some good studies that suggest that there is quite a lot of variation in the area so you may think ‘there is an artery here’ but actually, it’s somewhere else.
What are your final words of advice?
DP- Really try and identify the patient’s expectations and give them the real picture of the results that can be achieved. The most common request I get asked when treating the lips is to get rid of the deep lines – I tell patients that you’re not going to get rid of them, you’re going to soften them, and it’s important that they understand that.
JC – Don’t inject large amounts inappropriately – there is a lot of over injecting going on and that damages our speciality because it makes people think that it’s what the lips should look like.
ER- Make sure the function of the lips are kept – coming from a dental background, I am very concerned with maintaining the integrity and functionality of the lips – there seems to be a real desire to make lips look sexy by having a space in the middle, but they are designed to close the mouth and to keep the teeth healthy.
REFERENCES
1. AL-DREES, AM, ‘Oral and perioral physiological changes with ageing’. Pakistan Oral &
Dental Journal, 2010, 30(1) p.26-30.
2. Bodic F, et al, ‘Bone loss and teeth’. Joint Bone Spine, 2005, 72(3) p.215-221.
3. Sveikata KI, Balciuniene, & J Tutkuviene, ‘Factors influencing face aging. Literature review’,
Stomatologija, 2011, 13(4) p.113-6.